








Trunk recovery in stroke patients using 3D kinematic analysis: a useful tool to improve neurological rehabilitation.

Author: Marta Francisca Corrà, Ph.D.
The interest in kinematic characterization of impairments due to neurological diseases is based on the need to better understand the relationship between movement quality and performance after neurorehabilitation. Furthermore, it has been shown that 3D kinematic measures can help identify deficits even in individuals considered clinically well recovered [1] and is essential to differentiate between compensatory and non-compensatory movements [2]. For example, kinematic measurements have become a powerful tool to assess motor recovery in stroke patients [3].
Indeed, through kinematic analysis, various performance indices can be measured during the execution of movements; however, there is still no consensus on the most appropriate kinematic parameters to be used for the evaluation of trunk rehabilitation in stroke. For this reason, an Italian study conducted by the S. Anna Institute and Research in Advanced Neurorehabilitation (RAN) proposes a 3D kinematic protocol aimed at evaluating the validity of a kinematic system during trunk movements [4].
A total of 45 post-acute stroke patients were evaluated before and after intensive conventional neurorehabilitation treatment. An eight-camera system was used to analyze 3D trunk kinematics during typical movements (anterior/posterior and right/left lateral), particularly the Range of Movements (RoM). During dynamic seated balance, patients performed anterior, posterior and lateral (right and left side) displacement tasks (fig. 1).
The study found that several kinematic variables reflected motor recovery assessed with clinical scales. Standard neurorehabilitation treatments showed consistent improvement in all clinical and kinematic measures of the trunk (all p ‘s < 0.01). In addition, several significant relationships were found among the kinematic measures, and in particular, lateral pelvis was the only kinematic predictor of improvement in trunk motion.
In conclusion, the study showed that several kinematic variables reflect motor recovery assessed by conventional clinical scales. However, from the redundant variables provided by kinematic analysis, a single factor deserves to be translated into the clinical practice of stroke rehabilitation. However, it is necessary to take an integrated approach to the assessment of motor recovery, including clinical and kinematic assessments.
You can find the full paper at this link: https://doi.org/10.1016/j.medengphy.2020.01.013
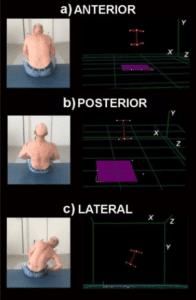
Fig.1 Kinematics of trunk during the execution of specific displacement tasks: anterior inclination; posterior inclination; and lateral displacement. Red lines represent 3D model reconstruction of the bodily kinematic markers.
References
[1] Karthikbabu S , Chakrapani M , Ganeshan S , Rakshith KC , Nafeez S , Prem V . A review on assessment and treatment of the trunk in stroke: a need or luxury. Neural Regen Res 2012;7(25):1974–7.
[2] De los Reyes-Guzmán A , Dimbwadyo-Terrer I , Trincado-Alonso F , Monasteri- o-Huelin F , Torricelli D , Gil-Agudo A . Quantitative assessment based on kine- matic measures of functional impairments during upper extremity move- ments: a review. Clin Biomech 2014;29(7):719–27.
[3] Levin MF , Liebermann DG , Parmet Y , Berman S . Compensatory versus noncom- pensatory shoulder movements used for reaching in stroke. Neurorehabil Neu- ral Repair 2015;30(7):635–46.
[4] Carozzo, S., Serra, S., Pignolo, L., Tonin, P., & Cerasa, A. (2020). The assessment of trunk recovery in stroke patients using 3D kinematic measures. Medical engineering & physics, 78, 98–105.
